



Expose The Young

23Mar: Sorry for doing this, but I found errors, & can’t stand to let them stand, so I’ve edited this substantially to fix them. The more features one adds to a sim, the more chances for bugs!
In my previous analysis of (voluntary) deliberate exposure (plus immediate isolation), I assumed that people were quarantined and exposed at random. But there seem to be good arguments for preferring either the young & health or the old & sick early. Exposing the old early gives them access to a less overwhelmed medical system, while exposing the young early allows the population to more quickly reach “herd immunity”, saving the old from later exposure.
To see which effect is stronger, I’ve changed my spreadsheet model to let the population be split into two groups who can differ in their death rate, and in whether they are quarantined or deliberately exposed.
As before, I start with one random contagious person in a US-sized population of 327M uninfected. After 7 days each contagious person becomes visibly sick, 10% of these need an average of 7 ICU days of help, and after 7 days some fraction of sick folks die, while the rest recover and are immune. Sick folks are added onto the usual 10K people who need ICU help each day, and their death rate goes as the log of the daily total number of people who need ICU help. If only 10K people total need ICU help, only 0.4% of sick folks die, but if 50K per day people need ICU help, then 3% of them die. (See below for alt death rate function.)
The number of infected people who become contagious each day is proportional to the product of the uninfected count times the contagious count. Except that there is a quarantine that always holds 10M people, with a proportion of contagious vs. uninfected the same as the larger population from which it is drawn. People in quarantine have only 2% leakage of the usual rate of infecting others. (See below for alt leakage rate.) The infection rate parameter is set so that, early on, the death so far count doubles about every 6 days.
To allow an old and a young group, I found US estimates on the population fraction and life-years remaining for different age and gender combinations, and also on how COVID19 death rates change by age, gender, and comorbidity. From these I’ve defined 72 groups which vary in age, gender, and a binary health-or-not, and produced estimates for each group on life-years remaining and COVID19 death rate. Sorting these groups by death rate, I can split them many ways into two groups: “young” with a lower death rate and higher remaining life-years, and “old” with a higher death rate and lower life-years. Depending on the cutoff between young and old, the ratio of their death rates varies from 36 to 6781, and the ratio of life-years remaining varies from 1.7 to 10.4.
I compared 8 options with varying combinations of who is quarantined: all (= random), young only, or old only, and also who is deliberately exposed: none, all (=random), old only, and young only. As before, I assumed a quarantine big enough to hold 10M, and that higher death rates induce higher needed ICU days. For each option I crudely searched to minimize the total lost life years by varying the young vs. old cutoff, the number of days of deliberate exposure (E days), and the fraction of the quarantine used for those deliberately exposed (D % of Q).
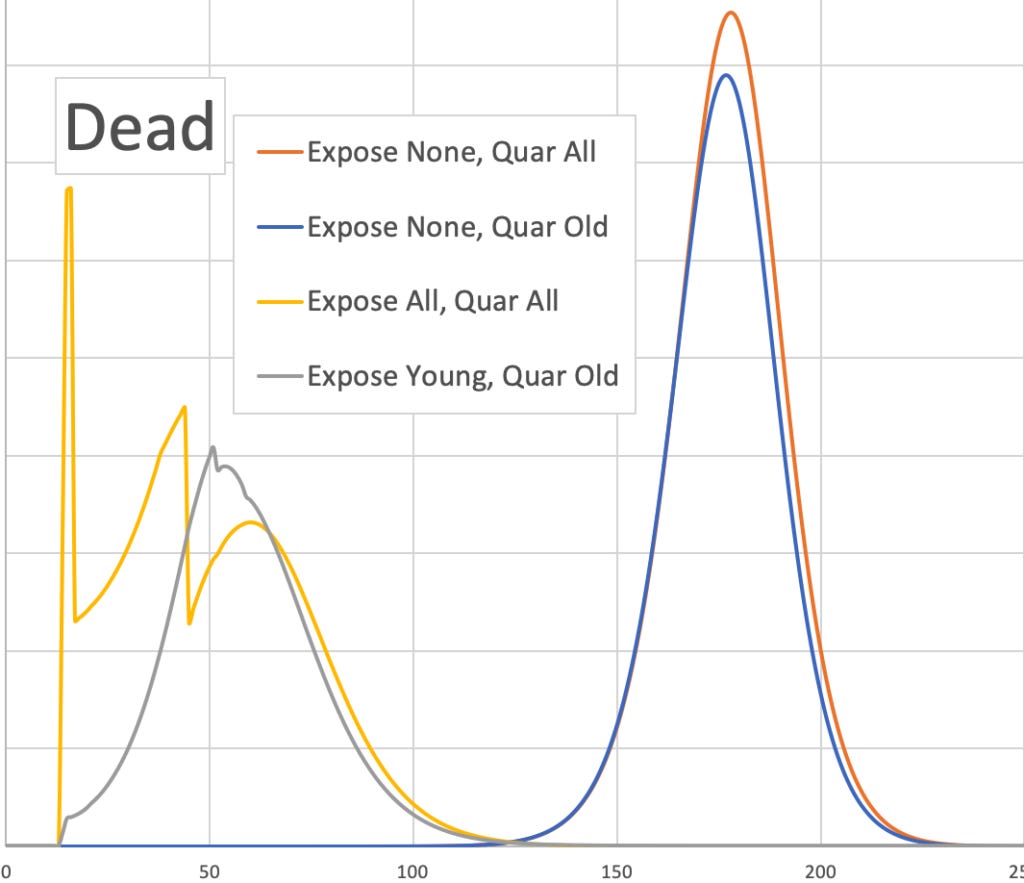
The following table shows my results, as do 3 graphs at the end of this post.
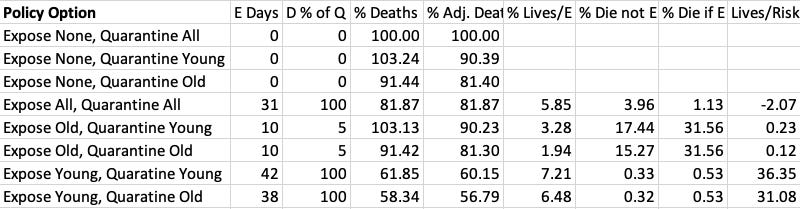
The 4th and 5th columns (% Deaths and % Adj. Deaths) give the percent of deaths, and life-year-adjusted deaths for each option relative to the first (baseline) option. Note that both choosing to deliberate exposed random folks, and choosing to quarantine the old, each save about 18% of life-years lost. Combining those policies, via quarantine the old and deliberately expose the young, saves about 43%.
For all but the last two options in the table, the optimal age cutoff had 24% being “old”: healthy men 60+ and women 65+, and also unhealthy men 40+ and women 50+. For the last two options, the optimal age cutoff had 26% being “old, adding in only healthy women 60-64.
The next three columns give percent chances of dying relevant for the deliberately exposed. % Lives/E is about the average % chance of deaths avoided in others per deliberately exposed person, relative to the same quarantine policy but no one deliberately exposed. % Die not E and % Die if E are about the % chances that someone would die if they die not or did become deliberately exposed. The last column Lives/Risk gives the ratio of the decreased chances of death in others over the personal increased chance of death in the deliberately exposed.
In the last two options which exposing the young, one can offer the young a dramatic motivation for choosing to become deliberately exposed. In addition to any cash compensation, or perhaps medical priority for loved ones, each volunteers to choose deliberate exposure saves someone else a 6.5-7.2% chance of death while themselves suffering only an additional 0.20-0.21% chance. And they can brag about having passed strict health requirements to be eligible. Much like a soldier at war, they can credibly claim to be an elite who made personal sacrifices to cause much larger community gains. (E.g., US soldiers in Iraq in ’06 suffered 1/255 death rate.)
Okay, I tried some variations to test robustness. I encourage you to try variations as well:
I tried increasing the quarantine leakage from 2% to 10%. Here quarantine old, expose none, gives 82% of baseline loss, while quarantine old and expose young has 77%. So a much leakier quarantine gives smaller, but still positive, gains to deliberate exposure.
I tried doubling the quarantine size, and found losses, relative to baseline, of 72.7% for quarantine old, expose none, 80.9% for expose & quarantine at random, and 40.7% for expose young quarantine old. So the gains of deliberate exposure increase with the size of the quarantine.
I replaced the log death function with a two-state function: The first 10K ICU cases per day get a low death rate of 0.4%, while any more get a high death rate of 3%. Results are quite similar. The optimal young/old cutoff turn out to be the same. Adjusted deaths for quarantine old is 82.4% of baseline, for exposing at random is 87.2%, and for expose young and quarantine old is 61.5%. In that last option, each young deliberately exposed saves 1.7% of another life, paying a personal added risk of .07% chance of death. So while the ratio is similar, both amounts are smaller.






I'm pretty aware that RobinHanson didn't include any economic aspects in the model (which, BTW, is even a PLUS in support of the "deliberate exposure" strategy) but, due to the huge economic impacts of lockdown measures, I guess no one can consider the 18 months period (the most frequent estimate for a vaccine) as anything "near-term". Even 12 months are not near enough for businesses and workers.
But if one could get all of them infected at the same time, it would be enough to have it 14 days before Spring Break, and still let them go...and even return to finish term at faculty!